Due to the glacial pace of evolutionary adaptation in many if not most ways, the genome could be considered a lagging indicator. It is tuned to invariants of a bygone regime – the environment of evolutionary adaptedness (EEA). Life would probably be not as robust and diversified if it had to solely rely on a mostly fixed genome and chance variation to navigate the dynamism, the danger, and the deception of the world. Thus, even a rudimentary ability for recognition, memory, and response would confer a selective advantage to any organism that evolved such a mechanism. The capacity to learn is that mechanism. Through evolutionary time, organisms that possessed the ability to learn had a better chance of surviving than those with fixed behaviors. Humans, endowed with the boon of an unlocked primate cerebral cortex, extended development, unparalleled cooperation, and a capacity for language are paradigmatic learners. We selectively attend to and interact with aspects of the world, we recognize patterns from these interactions, we use these patterns to make predictions, and then evaluate the accuracy of the prediction. Motivation, active exploration, attention, prediction, and error-feedback are the pillars of learning.
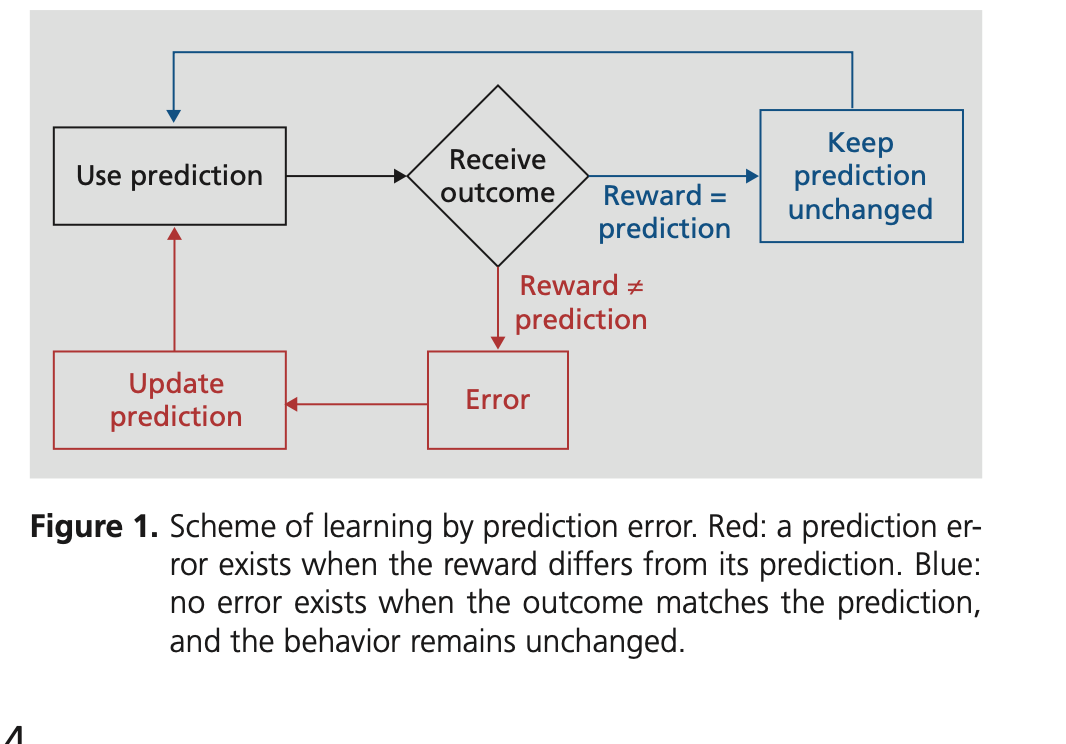
Trial-and-error feedback is a universal process for learning in the biological world. It is a mechanism of inferring causes from effects. Temporality and spatial proximity are prominent features in this process. If hearing a roar for the first time was followed by an unanticipated lion or seeing smoke nearby heralded a rapidly approaching fire, then the unexpected causes of those effects ramified those associations. In emotionally valent examples like above, the roar or the smoke will likely forever motivate action. In less emotionally charged situations, it is the repetition of prediction and error-feedback that incrementally reinforces associations. The brain-circuit in which predictive and error signals have been best demonstrated is the dopamine reward circuit, that not only responds to actual rewards, but also constantly anticipates it. Dopamine strengthens synaptic connections in a process of Hebbian plasticity and is colloquially phrased as “Neurons that fire together, wire together.”
In itself, the backpropagation of errors is an excellent mechanism for learning in niche constructed (upcoming essay), constrained, and well defined domains with clear error labels such as school-learning and game-playing. However, most sociobiological domains are not as rule-bound. Patterns and regularities abound, many irrelevant, some illusory, and a few intentionally deceptive. An undirected or unconstrained learning agent not only risks making false associations but also risks drowning in a sea of associations (next essay). Fortunately, biological agents are neither unconstrained nor unguided. They are limited by their sensory channels, memory, and response breadth. Also, at all times of development, they are tuned to learn the reward schemes of their local ecology and actively seek out that reinforcement. If rewards in the form of prediction errors drive learning, then expected rewards drive motivation. Beyond Darwinian drives and individual dispositions, humans are conditioned to the reward schemes of their culture and its institutions. Cultural reinforcement serves as a selecting mechanism to narrow the space of possible associations to a space of salient associations. Culture informs not only what to learn and what to ignore, but also provides the error-labels that direct learning.
As the culture of medicine has evolved from an art of treating the individual to a multibillion dollar industry for managing millions, its incentive schemes and source of error-labels have also changed. In that transformation, it is the population rather than the individual that has become the locus of analysis and attention. Under the strain of population health, the language, the culture, and the metrics of industry now permeate the practice of medicine. Measures of productivity (i.e. patients/hours), efficiency (i.e. door to doctor time), and profitability are enshrined on dashboards as key performance indicators that drive system and individual behavior. Evidence generated on unrepresentative populations in unrepresentative contexts with poorly defined diseases are prematurely sanctified under the banner of standards of care. Population level screening tests that do not consider more individualized risk-profile are creating a silent epidemic of false positives (next essay). A singular focus on “turning dashboards green” directs learning and behavior to that task and in turn blinds the system to other sources of information. In reality, the practice of medicine is informationally open with vast areas of uncertainty. Disease categories and patient categorizations are relatively crude or are not fit for purpose, so unrecognized patient level variation and miscategorizations can lead to unanticipated and counterproductive consequences at the individual and population levels. In a regime of complexity, top-down and rigid metrics can be premature because it standardizes behavior across the system, misdirects learning to a restricted search space, and leaves the system open to the unanticipated consequences of the unrecognized and unmeasured (next essay).
When the writer John Hersey wrote, “learning starts with failure” he was pointing to a universal mechanism that enables all organisms to survive in an infinitely complex and often hostile sociobiological world. However, knowing what to learn, what to ignore, and where to seek error-labels are just as important as the learning itself. Otherwise organisms risk being overwhelmed in false associations (next essay). Motivation in the form of expected rewards is the mechanism that ties learning to salient features of the environment. For humans those rewards are provided by culture and its institutions. In the era when medicine was an art, learning happened locally at the level of the individual patient and the physician. This bygone era has yielded to the era of industrial medicine, where the metrics tied to “population health,” productivity, and profitability enshrined on dashboards drive learning and behavior. The past in many ways was an era of medical barbarism. As Francis Bacon remarked, “the remedy [was] worse than the disease.” In the era of industrial medicine, the suffering continues, often delayed, many times slower, and hidden behind the veneer of science.
Discover more from S-Fxn
Subscribe to get the latest posts sent to your email.

[…] agents. These symbolic constructs direct attention, inform perception, bolster memory, scaffold learning, influence actions, and ultimately determine cognition (next essay). Our culture, although […]
[…] by allowing us to offload key cognitive capacities such as perception, memory, attention, and learning. Then, the question becomes what role do modern technologies play in contemporary errors of […]
[…] that is dripping with emotion and strained by cognitive overload. In a domain with significant knowledge gaps, where “noise” is often indistinguishable from “signal,” attention to […]
[…] As stated earlier, ‘testing at presentation’ is designed to cope with volume pressures and to satisfy metrics such as wait-times, length-of-stay, and patient satisfaction scores. Even though testing low-risk […]
[…] available, the use of risk-stratification scores is pushed top-down on emergency physicians. The perceived value of these tools comes from the fact that they integrate […]
[…] to be an active search process that serves as a time-sink. At best, the drive to efficiency and standardization with the development of one-click order-sets, copy and paste techniques, and templated […]
[…] It is laden with boilerplate language and codes designed to optimize billing, mitigate risk, and satisfy metrics. This in turn has led to documentation that is not only generic, depersonalized, and lacking the […]
[…] low value, and lacking explanatory power. In the modern era of industrialized, bureaucratic, and metric tyrannized healthcare, it is subjective and intersubjective information that becomes neglected, genericized, […]