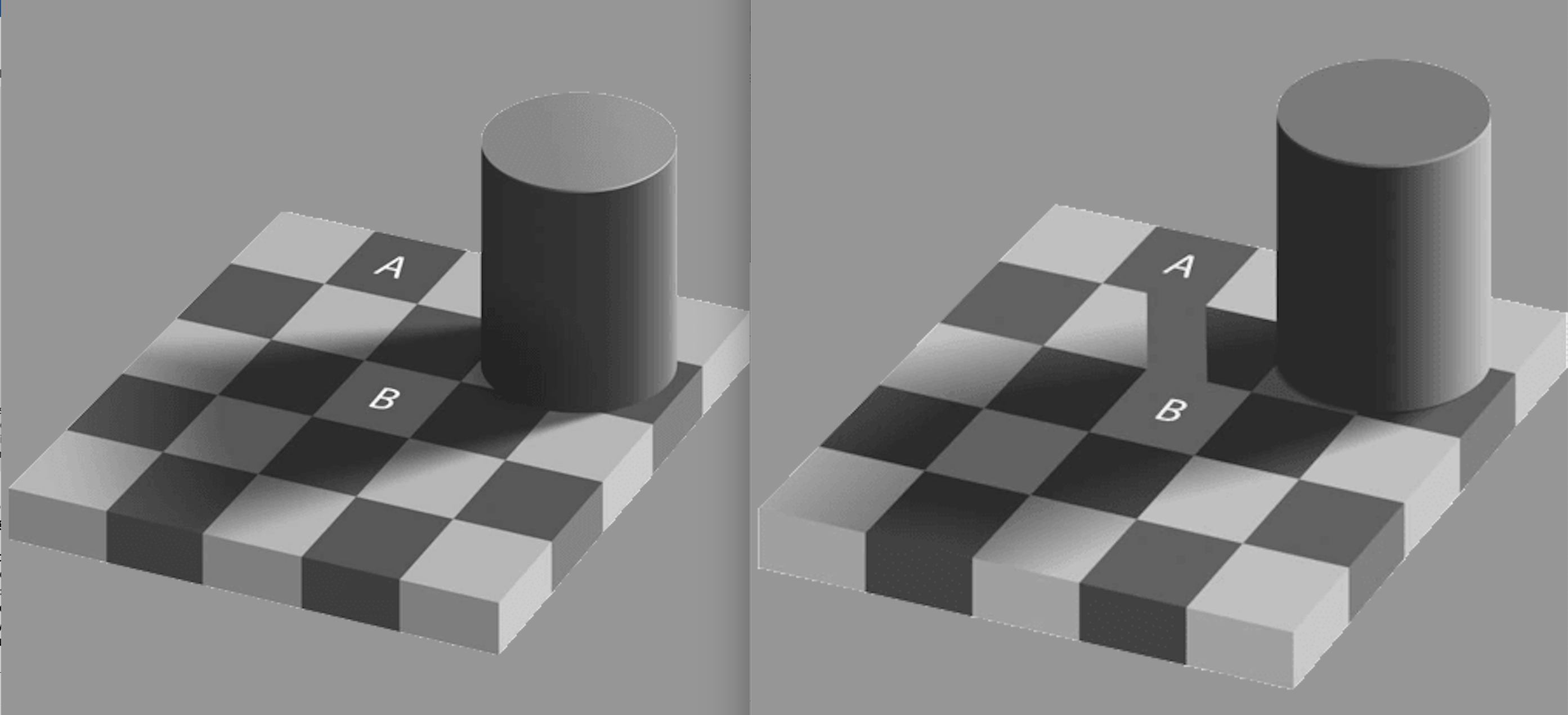
Visual illusions (see below) provide unique insights into the generative aspects of perceptions and the gaps between perception and reality. They not only illustrate the disproportionate impact our learned and innate knowledge of the world – our priors – have on our perceptions, but also that perception is not a direct reflection of the world but a filtered construction of that world. The brain is not a passive organ receptive to incoming stimuli, but in fact is an active, inherently predictive participant that utilizes innate knowledge, learned associations, and expectations in tandem with incoming stimuli to create a reality of affordances (future essay). When viewed within a Darwininian framework, this makes sense because perception only has to be high-fidelity or costly enough to discover organism-salient regularities in the environment. The organism only needs to only find what is important in the environment for differential survival and reproduction. Although, the end result is a feeling that our perceptions mirror the world, but in reality, even the simplest act of perception is predictive and involves assumptions, built-in knowledge, judgments, expectations, and interpretations.
This framework of “priors” influencing perceptions fits so strikingly into a Bayesian framework, that brain “algorithms” are considered by some to be fundamentally Bayesian. Bayes’ theorem states that the posterior odds of a hypothesis equal the likelihood ratio multiplied by the prior odds of the hypothesis. “Top-down” predictions driven by our priors interact with “bottom-up” percepts to create a prediction error. Minimizing this prediction error – by updating beliefs (priors) or changing what we do “see” or do not see – is what drives the process of perception. In fact, the tendency for confirmation bias, can be explained by the fact that it is energetically and cognitively less costly to ignore disconfirming evidence in favor of entrenched beliefs. These conditioned perceptions have implications for the delivery of care. Applied to the Emergency Department specifically (and possibly to the healthcare system in large), errant priors leads to systemic misperception of large groups of patients. Also, when these perceptions are reflexively coupled to imprecise, rules-based categorizations (future essay) based on superficial features, it can lead to systemic down-weighting of percepts leading to worse outcomes for segments of the population.
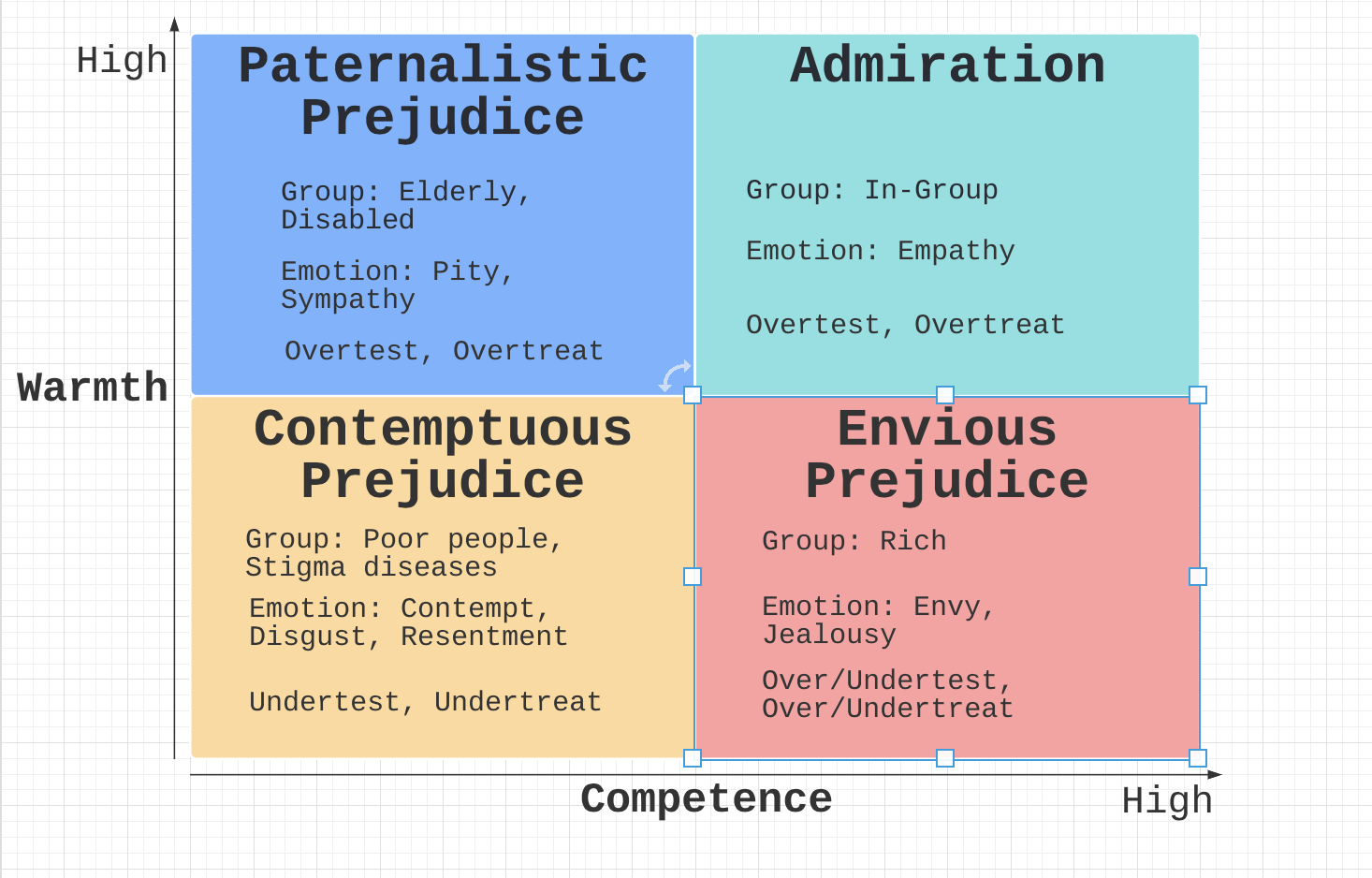
One social science model that provides a framework for interpersonal impression is the stereotype content model. It proposes that interpersonal impressions are formed along two dimensions: warmth and competence. These developed impressions serve as priors that inform perception. When applied to healthcare and electronic medical records, common descriptors such as “drug-seeking behavior,” “polysubstance abuse,” “opioid dependence,” “homelessness,” “disheveled,” “belligerent,” “agitated,” “foul smelling,” “elderly,” “frail,” “pleasant,” and “black male,” “obese female” lead to differential testing and treatments across the categories. For example, there is evidence that Black Americans are systematically under-treated for pain relative to white Americans. In general, it would not be a reach to claim that the “low warmth-low competence” group are under-triaged, have longer wait times, are under-treated, and mis-treated leading to poorer outcomes. Or that “high warmth – low competence” patients are over-triaged and over-treated leading to worse outcomes caused by iatrogenesis.
Furthermore, in frequently cognitively and affectively overloaded emergency departments (prior) – operating under the tyranny of imposed metrics (prior), the realities of revenue generation (prior), the specter of malpractice (prior), the optimization of the flow of patients (prior) – automating tasks and standardizing treatment plans is a necessity for survival. The downside of this strategy is that perception-action loops become increasingly reflexive, incoming evidence is down-weighted or ignored, and predominantly driven by priors leading to cascades of self-reinforcing and ultimately suboptimal decisions within and across encounters (future essay) leading to persistently poor outcomes for certain segments of the population. This risk has the potential to become even more magnified and systematized with the application of generative AI trained on health care system generated medical records (future essay).
The 18th century philosopher Immanuel Kant said, “perception without conception is blindness; conception without perception is empty.” The interrogations of science is showing us that in fact, neither is possible without the other. From birth, we perceive in the contexts of our priors (concepts), which in turn informs our priors in an endless loop. Additionally, since perception is the substrate of action, misperception can lead to reflexive and suboptimal decisions. I posit that errant perception – exteroception and interoception – plays a role in poor healthcare outcomes. Fortunately, individually and collectively, humans are not restricted by the perception-action loop but have the ability of metacognition (next essay) that can not only track errors but like a Bayesian can also calibrate confidence in their decision to the strength of the evidence.
Suggesting Reading:
Surfing Uncertainty: Prediction, Action, and the Embodied Mind
Discover more from S-Fxn
Subscribe to get the latest posts sent to your email.

[…] fluency. This impairs metacognition and can obscure the risk inherent in the under-differentiated, culturally heterogeneous, complex socio-medical Emergency Department patients who come with low-base rate, atypically […]
[…] and then evaluate the accuracy of the prediction. Motivation, active exploration, attention, prediction, and error-feedback are the pillars of […]
[…] in the hearts and minds of cultural agents. These symbolic constructs direct attention, inform perception, bolster memory, scaffold learning, influence actions, and ultimately determine cognition (next […]
[…] that predispose us towards fast and frugal decision making, superficial pattern matching, and retrospective narrative construction. These evolved dispositions no doubt play a role in our cognitive errors, but our cognition is not […]
[…] time, but mostly serves to facilitate an illusion of fluency. This in turn amplifies and ramifies perceptual biases, leading to the insidious effects of false positives and the more immediate consequences of false […]