Aging is the defined as the gradual functional and structural decline of an organism, resulting in an increasing risk of disease, impairment, and mortality over the life span. It is thought to be reliant upon a balance of 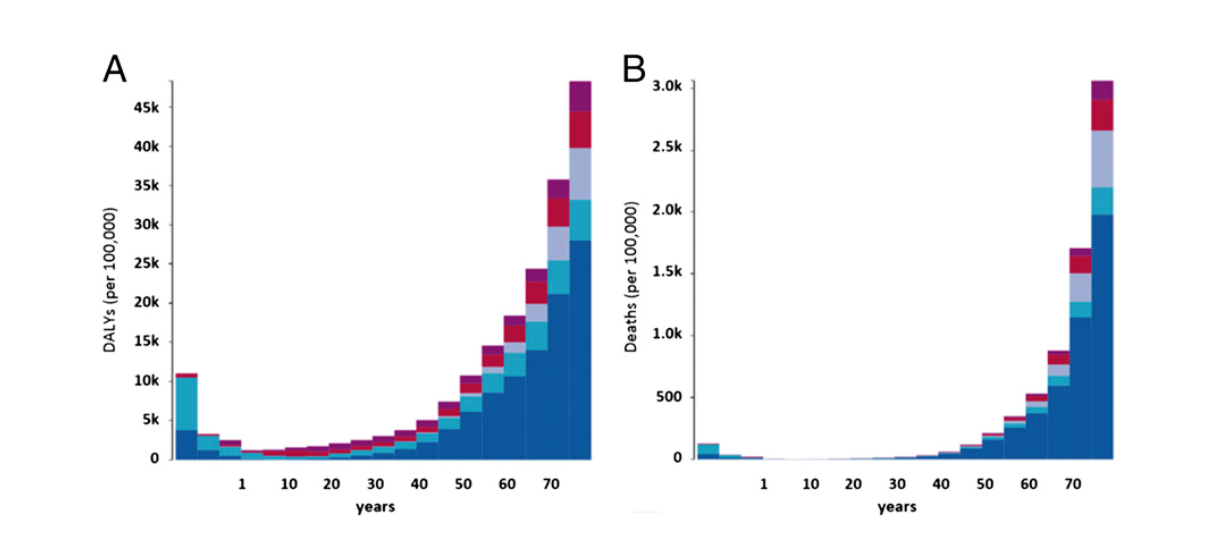 exposure and resiliency. By 2050, the world population aged 80 years and above will more than triple to approximately 400 million individuals. In the United States, it is estimated that one fifth of the population will be aged 65 and older. However, this increase in life expectancy will not come without a trade off. It is becoming abundantly clear that we have traded the decrease in mortality with an increase in chronic disease and its resulting disability. We are living longer but more of us are spending our retirement ages limited by the disabilities of chronic diseases. As you can see in the above graph, the toll of chronic disease begins to rise exponentially after the fifth decade of life as measured by disability affected life years (DALY).
exposure and resiliency. By 2050, the world population aged 80 years and above will more than triple to approximately 400 million individuals. In the United States, it is estimated that one fifth of the population will be aged 65 and older. However, this increase in life expectancy will not come without a trade off. It is becoming abundantly clear that we have traded the decrease in mortality with an increase in chronic disease and its resulting disability. We are living longer but more of us are spending our retirement ages limited by the disabilities of chronic diseases. As you can see in the above graph, the toll of chronic disease begins to rise exponentially after the fifth decade of life as measured by disability affected life years (DALY).
However, chronological age is not the most reliable indicator of the body’s rate of decline or physiological breakdown, but at best, serves as a proxy for the rate of aging. Models of biological or fitness age are much better predictors of all cause mortality and morbidity. Biological age estimates facilitate the merging of multiple biomarkers into a single latent variable. Nevertheless, currently there is no consensus regarding the components of this metric nor have the validity of any of these measures have been validated. In contrast, cardiorespiratory fitness (CRF) via measured VO2 max and even calculated VO2 max are excellent predictors of cardiovascular disease and premature all – cause mortality. CRF may actually be a stronger predictor than traditional risk factors such as weight, high blood pressure, smoking, and aberrant cholesterol profiles but a single CRF measurement in addition to the above risk factors considerably improves risk classification of individuals. Additionally, improvements in CRF are associated with risk reduction, and most importantly, the largest benefit is observed between low and medium fitness groups. In other words, going from a low fitness state to a medium fitness state has the largest decrease in mortality risk.
As I mentioned in an earlier blog, improving physical fitness (rather than weight loss) should be the primary objective of medical recommendations and public policy. Even small gains in aerobic capacity has long lasting and more predictable effects on mortality rates than inadequate metrics such as a decrease in BMI. Additionally, improvements in CRF are measurable, attainable, and sustainable because it requires a moderate intensity level. In contrast, weight loss requires us to not only overcome the evolutionary constraints of energy conservation but more importantly, necessitates us to overcome the cultural constraints that makes energy expenditure a “to do” item and energy consumption something to “control” on a daily basis. Furthermore, even if we are able to exert such discipline, weight loss is often not forthcoming and linear. Therefore, weight loss for the majority of the population is at best short lived and unsustainable. For the foreseeable future, mortality rates will always be a hundred percent (as we all have to die), however, goals of improving CRF is currently the best, most effective method for decreasing DALYs, and thereby, increasing an individual’s and a population’s quality of life.
Discover more from S-Fxn
Subscribe to get the latest posts sent to your email.

What do you recommend to be the most effective way of losing weight and sustaining the loss?
[…] risk factors were found to account for ~40% of the attributable disability-adjusted life-years (DALYs) worldwide. If you take the example of diabetes and consider glucose intolerance, pre-diabetes, […]